
Diagnosing ALD
It is essential to diagnose ALD as early as possible. All the evidence indicates that the two currently available treatments for the disease -- Lorenzo's oil and stem cell transplantation -- only work during a very narrow window either before symptoms develop, or very early after their onset. Once the disease has progressed and symptoms have become severe, there are currently no treatments that can replace the lost myelin and the only treatments available are palliative.
Unfortunately, cases of ALD are often missed or misdiagnosed during the critical period of early onset. This is often because diagnosing ALD can be a tremendous challenge for many physicians. The earliest symptoms of the disorder in childhood can easily be mistaken for a number of other, much milder and much more common developmental and behavioral problems, such as attention deficit disorder (ADD/ADHD) or learning disabilities.
What Should Parents and Families Look For?
It is very difficult to differentiate ALD from other conditions, such as ADHD, epilepsy, autism, and other learning disabilities, particularly if you are not aware that a genetic predisposition to the disease runs in your family. However, if you notice some of the following things, be sure that your child's physician is considering the possibility of ALD -- especially if you have a family history of neurological problems:
Late-onset ADHD or other attention problems.
A child with ADHD usually shows attention problems in preschool or early school years, while ALD symptoms appear between ages six and 10. If your son had no trouble paying attention in kindergarten but is suddenly developing problems in second grade, mention this to your doctor.Lack of response to medications for ADHD.
If your child has been receiving a stimulant medication for ADHD and has not responded, your doctor will probably suggest a change of dose or change of medication. Ask for a blood test for ALD and a brain MRI at the same time.Adrenal insufficiency.
If your doctor diagnoses your child with Addison's disease, a test for ALD should be automatic, since ALD is the most common reason for Addison's disease in childhood.Problems with vision.
Visual impairment, caused by lesions on the optic tract, is characteristic of early seen ALD, and is frequently misdiagnosed.
Diagnosis through newborn screening
If you receive an ALD diagnosis via newborn screening, please watch this video.
Most US states now test all newborn children for ALD.

Image courtesy of the ALD Alliance
What Should Physicians Look For?
Some key clues that should alert physicians to consider the possibility of ALD include:
A family history of significant medical conditions, early morbidity, or symptoms of behavioral or developmental disorders that appear to be genetic;
Signs of abnormal development in the child;
Changes in the child's functioning, such as declines in cognition, learning, behavior, or emotional regulation;
Rapid acceleration of such changes;
Late onset of symptoms that typically occur earlier in childhood, such as attention or learning problems;
Visual-spatial or visual-perceptual difficulties; and
Lack of sustained response to symptomatic therapies.
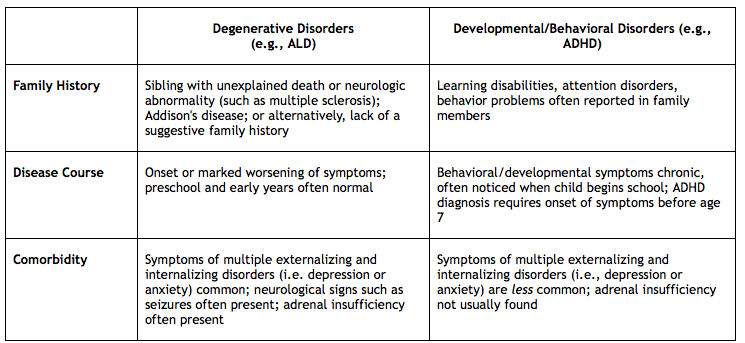
Physicians may consider referring to the following table when ALD is included as a differential diagnosis:
MediView Report!
Read the MediView Report, Avoiding the Misdiagnosis of Adrenoleukodystrophy: Distinguishing ALD from ADD/ADHD.
Diagnostic Testing
Once ALD is suspected, there are two tests that must be done: a blood test and a brain scan. The blood test analyzes the amount of very long chain fatty acids, which are elevated in ALD. This test has the highest degree of accuracy in males; however, it can sometimes miss the presence of the mutated gene in women who are carriers of the disease.
If the blood test suggests ALD, a magnetic resonance imaging scan (MRI) will be performed to determine if the disease has begun to do damage to the brain. Lesions on the brain caused by the destruction of the myelin will appear on MRI before any neurological or psychological symptoms appear. The MRI scan will produce something called a Loes score, which rates the severity of the damage to the brain on a scale from 0 to 34. A score of 0.5 or less is normal; a score of 14 or more indicates severe ALD.
Genetic Testing
When a child is diagnosed with ALD, among the first questions many families ask are "Are our other children at risk?" or "Can we safely have more children?" Genetic testing is the only way to answer that question. DNA-based blood tests can accurately identify both women who are carriers of the gene, and boys and young men who have ALD and may not yet be showing symptoms.
Research shows that screening not just the parents and siblings of boys with ALD, but extended family members as well, is the best way to detect the disease at a time when treatment can be beneficial.
Although it is not currently feasible to screen all pregnant women for the ALD mutation, prenatal tests and genetic counseling are available to help families plan their pregnancies and avoid passing the ALD gene on to their children.
Amniocentesis and chorionic villus sampling (CVS) can both detect the ALD abnormality, but only if testing laboratory or physician is specifically looking for it.
Doctors can contact the Kennedy Krieger Institute to request genetic testing.